Renal Services at St. James University Hospital, Leeds
Renal Services at SJUH commenced in the late 60s and comprised inpatients situated in Ward 33 on the upper floor of Beckett Wing and a dialysis and transplant unit on part of the ground floor of A block in Lincoln Wing. Ward 33 was split equally between general medical patients, under the care of Dr John Stoker, and nephrology patients. The dialysis and transplant facility occupied part of what was originally Ward 1 and consisted of two single rooms and a four bedded bay for transplantation and a Poulson designed wooden sectional porta-cabin like building constructed at the back of the wing housed the dialysis facility. This was established mainly to train patients in the technique of home haemodialysis and consisted of ten beds. There was also a small area which could be used to isolate patients if required. The office accommodation was Spartan in that there was a consultant’s office in the main block and outside the back door a caravan divided in two provided offices for the secretary and the junior medical staff.
The transplant unit, under the direction of Professor Geoff Giles, was quite inadequate as, apart from that mentioned above, there was nothing else, not even a patient’s toilet which was remarkable given that the aim of transplantation was to restore renal function. The nursing facilities were also sparse, the nurse’s station was situated in the four bedded bay as was all the necessary consumables. The patient accommodation was directly off the main corridor to the dialysis unit and so there was no possibility of nursing patients in any form of isolation. Given the risk of infection at a time when much higher doses of steroids were in use this was a significant problem. The unit was remote from the surgical wards and so the day to day management was supervised by the renal unit junior medical staff. It is just as well that at this time the number of patients being transplanted was rather few, twelve in 1994.
The first consultant was Dr Stanley Rosen who in the early seventies emigrated to America and the unit was subsequently managed by the locum appointment of Dr Brian Keogh. Dr Alexander (Sandy) Davison was appointed in 1974, from a general medical Senior Registrar post in Edinburgh, and took up post in June of that year. At that time the staffing consisted of one consultant, two registrars and two senior house officers to cover the inpatients, the dialysis unit and the medical cover for the transplanted patients. In the dialysis unit there were three sisters, Pat Farrer, Joan Wilson and Jenny Tirvengadum; a home dialysis sister, Jose Williams; four medical physics technicians led by David Evans, artificial kidney assistants and dialysis orderlies; a medical social worker (Dusty Gregg) and a dialysis administrator (Geoff Mason). The artificial kidney assistants were responsible for preparing the machines for dialysis and the dialysis orderlies stripped down the Kiil dialysers after each session and made them ready for the following session.
In keeping with many other services at the time there was little or no co-ordination across the city between SJUH and the LGI. For general medical and surgical emergencies the LGI accepted patients on even days and SJUH on odd days. For specialist services, such as renal medicine, both hospitals were open every day and as a result the two renal consultants in the city did not have any time when they were not supposed to be available for emergency admissions although each had reciprocal appointments to both hospitals. A situation difficult to imagine in current times.
The patient activity in the mid-seventies was rather meagre by comparison with today’s numbers. There were significant financial restrictions and generally dialysis was only offered to adults up to about the age of forty-five and to those who had no other intercurrent serious medical problems. Now this seems strange but at the time the technology of dialysis was still being developed and experience was being gained in clinical management. In 1975 some 27 patients were accepted to the dialysis programme at SJUH and 18 patients were transplanted. In the dialysis programme 12 were successfully trained in home treatment and 16 patients unfortunately died. In keeping with the experience of other units at the time, of the 18 patients receiving a transplant two died and four returned to dialysis within the year. A sixty-six success rate was considered very good as this was a time when immunosuppression solely consisted of prednisolone and azathioprine and tissue typing was still in its infancy.
As mentioned the emphasis was on training patients to undertake their treatment at home wherever possible. This was not universally achieved as patients’ home accommodation was not always suitable either as it was too small or it was difficult to access, one patient lived at the foot of a cliff on the North Yorks coast. There was an additional problem as the unit served a vast area which consisted of all of West Yorkshire, a part of North Yorkshire and some of what was East Yorkshire, a population of approximately five million. Each district had its own planning rules and regulations with respect to water supply, building regulations and, indeed, everything which was required to install a home dialysis facility. The majority were room conversions requiring sufficient space for the machine, consumables, water treatment and the cleaning, dismantling and rebuilding of the dialyser in preparation for the next dialysis session. Patients and relatives were trained to set up the machines prior to each treatment session and to dismantle the apparatus at the end. Vascular access was most commonly by the use of a Scribner shunt. This was surgically constructed by inserting a Teflon tip (a small hollow tube) into the radial vein and connecting it to a siliconized rubber tube with a similar device inserted to a suitable vein, usually the cephalic vein. These could then be connected together so that blood flowed from the artery to the vein. Dialysis access was then achieved by disconnecting both so that the blood flowed from the arterial end to the dialyser and then returned to the vein. This was a practical solution but not without its problems such as infection and intermittent clotting. Patients had to be trained in strict aseptic techniques but in spite of the best efforts such devices had a limited life, longer for those inserted in the forearms and significantly shorter for those in the lower limb. Subsequently arterio-venous fistulae were introduced and the patients or their relatives trained in needle puncture.
At this time dialysis was conducted with Kiil boards using cuprophane membranes. There were three boards – top, middle and lower. Cuprophane membranes were inserted between the boards in a sandwich arrangement and carefully bolted together. Ports were inserted so that the patient’s blood could be pumped over the membranes whilst the dialysis fluid was pumped in a counter direction on the other side of the membrane. At the end of each session everything would be dismantled, washed and re-assembled ready for the next session. The integrity of the dialysis membranes was pressure tested to ensure that there were no leaks between the blood compartment and the dialysis compartment. Such leaks resulted in a loss of blood for the patient which could be ill-afforded in an era prior to erythropoietin and when many patients had haemoglobin frequently 50% of normal. Typically treatment sessions lasted ten to twelve hours twice weekly. The first design of the Kiil boards had parallel grooves running along the length of the board as it was considered any turbulent flow may cause haemolysis. A design change was introduced by having the surface of the board with grooves running both the across and lengthwise resulting in a surface of very small pyramidal points – the so-called multipoint dialyser. This improvement in the interior design of the Kiil boards and the addition of a third layer blood compartment resulted in much improved efficiency such that each dialysis session could be reduced to six hours. Initially this was twice weekly but further experience led this to be reduced to four hours but undertaken thrice weekly. The consequence of this was that more patients could be accepted for dialysis. Initially the ten-bedded unit could accommodate a maximum of thirty patients – ten to twelve hours treatment twice weekly. With the reduction in dialysis duration each machine could be used twice daily and latterly thrice daily. Patients were treated on six days of the week; the remaining day was used for routine maintenance.
In the seventies peritoneal dialysis was not routinely used for maintenance treatment except in exceptional circumstances. Twice weekly peritoneal dialysis using a hard catheter was provided for a patient from the LGI unit who had run out of suitable sites for vascular access. This was not an uncommon problem in the early days of dialysis. A number of patients died from lack of vascular access. This was alleviated by two developments. One was the introduction of the arteriovenous fistula, the so-called Cimino-Brescia fistula, which allowed for the distention of suitable veins which could then be needle punctured on repeated occasions. The second was the development and introduction of Gore-Tex(R) grafts and techniques of vein grafting and including vein transposition and the use of umbilical cord veins. Mr Ralph Kester of the Department of Surgery was instrumental in developing the vascular access service and assessing the suitability of novel materials suitable for repeated puncture .
In 1976 Dr Davison and Mr Geoff Mason, the Home Dialysis Administrator, convened a meeting with the planning officers of all the districts where there were dialysis patients to see if a common planning policy could be adopted to reduce the time, cost and effort taken to establish patients on home treatment. Fortunately this was successful as a universally agreed specification for home haemodialysis facilities was adopted and the transition from hospital to home became significantly easier. A further advancement at this time was the development of a porta-cabin dialysis unit which could be placed in the garden of a patient. This had a number of advantages. It reduced the cost of adapting a room within the house, removed the odour from the family home of the sterilising solution and it allowed for the transfer of the facility to another patient should the existing patient receive a successful transplant. The cost savings were also significant as room conversions were somewhat expensive as was the costs of restitution of the room after it was no longer required. Once a patient was established on home treatment they were suspended from the transplant list for six months. There were no objections to this as the number of transplants were few and, in addition, it allowed patients freedom to choose their dialysis time to suit themselves and their family as well as relieving them of having to travel from home to the unit twice or thrice weekly. Sometimes it was difficult to install a porta-cabin due to the closeness of neighbouring houses and the Royal Air Force, on more than one occasion, was called upon to provide a helicopter to lift the cabin over the house and into the back garden. This was quite an operation calling upon co-operation between the installing team and the police and fire services for safety reasons.
Although functional, the facilities for renal services were in many ways quite inadequate. Inpatient beds in Beckett Wing and dialysis and transplantation in Lincoln Wing. On one occasion during winter a junior member of staff suffered significant injuries by slipping on ice covered steps whilst running outside to Beckett Wing to answer a crash call. Patients with acute renal failure were occasionally accommodated in one or other of the transplant unit’s single rooms. This allowed easier access for dialysis support but for those patients housed in Ward 33 they had to be transported by internal ambulance to the renal unit for dialysis. As a result plans were formulated to significantly upgrade to the facilities and eventually to bring the service together on one site. Although planning was started in 1974 it was many years later before a fully integrated unit was built and commissioned.
In the seventies there were financial restrictions on dialysis and this resulted in many charitable groups providing funds and equipment. The Leeds Kidney Research Fund, subsequently the Yorkshire Kidney Research Fund and now Kidney Research Yorkshire, was established by relatives and friends of dialysis and transplant patients. The purpose was to raise funds for dialysis equipment and to support research activity into renal diseases and treatment modes. It was initiated by Mot Bloom, a pharmacist whose wife had died from renal failure, and a committee was formed which met monthly and raised money for its activities. This was a very informal group who used to meet on a Sunday evening in Mot Bloom’s house with tea, cakes and cream buns provided. They achieved much raising sufficient to fund the salary of research fellow the first of which, Dr Geoff Walker, was appointed in 1976. Dr Davison was of the view that the NHS should be responsible for the funds required for treatment and persuaded the YKRF to concentrate on raising funds for activities not supported by the NHS and as a consequence the funds available for research increased significantly.
Other groups supported the unit. The Wetherby Lions Club through the good offices of David Brown raised sufficient funds to provide two mobile phones for the unit – one for Professor Giles and one for Dr Davison. These phones were quite unlike those in use now as they were of a considerable size, did not have a long battery life and did not have universal coverage. They were, however, very useful and significantly improved communications particularly during the arrangements with patients and staff when a transplant became available. The Rotary Clubs of Yorkshire were also very supportive. In the seventies dialysis equipment was cumbersome and not readily portable and so it was difficult for a patient to go on holiday unless they could be accommodated in another unit. This frequently proved impossible to arrange as most units were working to capacity and so had no spare space. In addition a number of units had experienced hepatitis infections with devastating effects on both patients and staff. At this time there was no hepatitis B vaccination available and so many units were reluctant to accept visiting patients from other units. The Rotary Clubs of Yorkshire led by the Scarborough Club gathered funds and bought a house in Scarborough in which a room was converted to accommodate a dialysis machine and the necessary equipment. This was subsequently maintained by the Yorkshire Kidney Research Fund and holidays arranged through the Home Dialysis Administrator at St James’s. This provided a much needed facility for patients but clearly was restricted to those who could undertake their own treatment but, at least, it allowed them to get away with their family and many took advantage during the summer months and during the festive season. An attraction was that the holiday home overlooked Peaseholm Park and so there were leisure activities nearby which was clearly of benefit to patients with young children. In May 1976 a similar facility was opened in Ilkley thanks to the efforts of the Ilkley Rotary Club. Unfortunately this second home never achieved the level of use as that of the Scarborough facility perhaps as it was situated closer to patient’s homes and thus did not provide the same appeal as getting away to Scarborough. The use of the Ilkley home was extended to other units but the uptake was minimal and so the dialysis facility was closed and the home returned to the Rotary Club.
The seventies saw the development of collaboration with other disciplines in Leeds. Joint paediatric clinics were established with Professor Roy Meadow and Dr Trevor Brocklebank at Seacroft Hospital and this was particularly useful for children transitioning to the adult service at SJUH. The combined clinics were held on the first Wednesday of each month and proved very popular with children and their parents. There was collaboration with Dr Munro Peacock and Professor Maurice McLachlan of the Department of Bone and Mineral Metabolism of The General Infirmary at Leeds. This resulted in much needed research into the bone problems experienced by many patients with renal failure, particularly children. Studies at this time related to the introduction of novel Vit D preparations which were just becoming available at this time. Joint clinics were held at SJUH and much expertise was obtained in the use of these new medications in the treatment of renal osteodystrophy, particularly in children. The SJUH renal unit was also recruited to the Medical Research Council’s Working Party on Glomerulonephritis and served as the centre receiving information from a number of units throughout the UK providing information on renal biopsies. This resulted in a number of publications and also the selection of patients for controlled clinical trials.
In view of Dr Davison’s background in pathology he established, in collaboration with the University Department of Pathology, a monthly review meeting of renal biopsies. This was a useful training opportunity for junior staff in renal medicine and pathology. This was enhanced by the appointment to SJUH of Dr Sam Aparicio and subsequently, following Sam’s retirement, Dr Barry Hartley. Initially only light microscopy was available but in time immunofluorescence and electron microscopy was added. This significantly enhanced patient management.
In 1976 a number of patients developed unusual neurological features. It most commonly presented with a speech disorder, slurring of words and stuttering, progressing to dysarthria and eventually mutism. This was accompanied by myoclonus, grand mal seizures and variable neurological deficits – twenty patients developed this syndrome. It was interesting that this was confined to patients on home haemodialysis and one of the SHOs, Dr Marion Sloan, mapped out the geographical distribution of the patients and found that they all resided to the west of Leeds. At this time there was suspicion of a link to aluminium toxicity. Aluminium was used as a phosphate lowering agent and was also used by water supply companies for the clarification of drinking water as it acts as a flocculating agent. Fortunately Yorkshire Water had detailed records of the monthly aluminium content of the water supply to each of the home dialysis patients and it became obvious that there was a clear link between the cumulative exposure to aluminium and the time taken to develop what became known as dialysis dementia. This was in agreement of data published from the Sheffield unit by Dr Margaret Platts. Transplantation did not improve outcome and, indeed, some patients developed symptoms following transplantation. The solution to this distressing syndrome was to install reverse osmosis water treatment to all the home dialysis installations and after this was done no new cases developed. Aluminium is not the only agent added to water supplies and little is known of the potential for diffusion of added chemicals across dialysis membranes.
In 1977 Dr Davison, Dr Frank Parsons and Professor Meadow arranged a conference to celebrate twenty-one years of dialysis in Leeds. This was an international meeting held at Bodington Hall, University of Leeds, with contributors from throughout the UK and Canada, France, Germany, Italy and Switzerland. This provided an up to date account of haemodialysis practice including vascular access and covered both adults and children. The proceedings were published in Dialysis Review by Pitman Medical and edited by Sandy Davison. The conference was sponsored by the Yorkshire Kidney Research Fund and by generous donations from thirty-two commercial organisations associated with dialysis. It was a considerable success and, surprisingly, Dialysis Review sold over 500 copies in the first three months from publication. It was a fitting tribute to the pioneering work of Frank Parsons in the field of dialysis.
In the seventies there were few patients on dialysis and so it was unusual for a general practice to have a patient being treated. This led to a number of problems as most general practitioners were unfamiliar with managing patients with either significantly reduced or no renal function and the subsequent need to alter prescribing habits for medications with renal elimination. A consequence was that for many patients the staff of the renal unit became their general practitioner. Although this was a functional solution it added to the workload of patient management. Dr Davison set up a number of teaching sessions where the clinical aspects of renal failure, dialysis and transplantation could be discussed. This proved useful and improved communications between the hospital staff and general practitioners.
The workload of the unit continued to grow and it soon became obvious that the existing facilities were inadequate even with an active home dialysis programme. Consideration was given to the establishment of satellite units where a number of patients could be treated. This had obvious advantages in that it could significantly reduce travelling time to and from treatment. At this time patients were drawn from as far afield as north of Scarborough in the east and half way to Manchester in the west. In view of patient density consideration was given to establishing a unit in Bradford but no suitable accommodation could be identified. After much searching space was found in what was an old stable block in Bootham Hospital in York, an old psychiatric Hospital, and this proved most suitable as it was relatively close to the centre of the town and had suitable parking space. Dr John Hutchinson of the Regional Health Authority was most supportive of this venture which proved very successful. This led the way to expanding renal services and facilitating the increasing numbers of patients being accepted for dialysis. Subsequently similar units were established in Bradford, Dewsbury, Wakefield, Halifax, Huddersfield and at Seacroft Hospital in Leeds. All were different due the type of accommodation available. In Bradford the building identified was an old dairy situated outside the back door of Bradford Royal Infirmary, interestingly one of the first patients treated there recalled as a young boy collecting milk from that dairy. In Wakefield a spare ward in an existing hospital was available. These facilities were established for all patients in Leeds but none were transferred from the LGI unit until the Seacroft facility was opened in 1999.
The satellite units were crucial in coping with the increasing numbers of patients receiving treatment but, in addition, they established a renal presence in areas remote from Leeds and led to the appointment of Physicians with an Interest in Renal Medicine in District General Hospitals and in time the transfer of these satellite units from SJUH supervision to other Health Authorities. This was to the advantage of District General Hospitals as it reduced the need to transfer patients to either of the Leeds Teaching Hospitals and established local renal expertise.
In May 1980 the Clinical Sciences Building was opened and the Yorkshire Kidney Research Fund supported the staffing and equipping of a renal research laboratory. This was accompanied by the appointment of a research scientist and research nurse.
In the seventies it was difficult to provide dialysis for children owing to the lack of suitable equipment being commercially available. Dialysers were designed for adults and it was technically difficult to dialyse patients who weighed less than 15Kg, due to the volume of the dialyser and connecting tubes. Things came to a head when the parents of a child in Seacroft stated that they would move to another part of the country where paediatric dialysis facilities were available, if necessary, if we did not start dialysis for their child. Fortunately this was at a time when there was a move away from reusable Kiil dialysers to disposable equipment some had smaller internal volumes and therefore suitable for children. Thus children joined with the adults being treated in the St James’s unit. This was a success in that the adults supported the children and the children brought much fun and enjoyment to the adult patients.
The development of disposable dialysers reduced the use of Kiil board dialysers but they were significantly more expensive. This was, in part, off-set by reducing the need for dialysis orderlies to strip and build the Kiil boards. The new dialysers consisted of capillary tubing housed in a plastic case and they came in varying sizes and differing material. This led to the possibility of treatment being tailored to individual patient requirements.
In 1980 with the opening of Chancellor Wing surgical patients were transferred from Lincoln Wing. The hospital matron and other administrative offices were also moved out to new offices and thus space became available in A Block to provide better offices for the renal unit medical staff. In addition a ward on the first floor also became available for the development of a dedicated transplant unit with four single rooms and appropriate supporting facilities. This was a significant and long overdue improvement in transplant services. In addition space was available for a paediatric dialysis facility on the first floor with paediatric trained staff appointed and led by Charge Nurse Philip Haines. The children appreciated their dedicated area but the adults were somewhat sorry to lose their companionship. A teacher was also employed to ensure that the children did not fall behind in their education as a result of them having to attend hospital three times weekly. In time other supporting paediatric staffs was appointed. Dr Trevor Brocklebank provided medical care and he was subsequently joined by Dr Maggie Fitzpatrick.
An innovative development was the provision of holidays for the paediatric patients. Each year staff and patients would go to a holiday centre taking with them all the necessary equipment and consumables. This provided a welcome break for the children but the staff often returned exhausted! On one occasion whilst in the south of England they even managed a day trip to France. An added advantage was that it allowed the parents of a child on dialysis a welcome break and afforded them time to spend with their other children.
In view of expanding services and additional consultant post was funded and Dr Es Will was appointed in 1980. He brought additional expertise to the unit with his interest in computing. This significantly improved data handling and he became nationally and internationally known for his IT skills. He arranged a seminar entitled Computing in Renal Medicine: Research and Routine and went on to contribute much to the UK Renal Registry.
By the late 1980s the unit was amongst the largest in the UK and as a result attracted visits from politicians. One minister of health wanted to see the transplant service and she was taken to see one recently transplanted patient. Dr Davison introduced the visitor to the patient saying “May I introduce you to Linda Chalker, the Minister of Health, who is visiting today”. The visitor held out her hand and said very pointedly “Virginia Bottomley”. On another occasion Edwina Currie visited and when Dr Will explained to her how the dialysis stations were being used to maximum capacity she looked up and said “I see five members of staff and three are overweight”. Politicians seem more concerned with photo opportunities and sound bites than meeting with patients and discussing real problems. The exception to this was Hiliary Benn, the Labour MP for Leeds Central, who took an active interest in the unit.
Early in 1980 a project team consisting of medical, surgical, nursing and technical staff was established to plan a new renal unit. This had a very prolonged gestation as no agreement could be reached as to where the unit was to be sited. A number of options were put forward but were all rejected for a variety of reasons. There was space identified to the west of Lincoln Wing but the ground was deemed to have too much of a slope to be a suitable site. It was not till it was decided to demolish the buildings behind A Block of Lincoln Wing that the new unit became a reality. Although the project team had been established in 1980 it was not till 1994 that the building of the new unit was accomplished.
The new unit was quite unique. It was decided to bring together both inpatients and outpatients as well as adults and children. The design was based on a nucleus design involving three nucleus templates. This design was not ideal but with much thought and discussion it proved possible to fit in all that was required. This was not without its problems. It was suggested to the Regional Health Authority that the design team should come and spend some time in the existing unit to see how the unit functioned and how the flow of patients, equipment and consumables could be facilitated. This was considered inappropriate as we might influence the architects and result in a greater building cost. The project team were at pains to explain the need for wide corridors as many patients required to be transported from to ward to the dialysis area on their bed. We were advised that regulations at the time specified that circulation space could not exceed 13% of the total area. Hours were spent in planning and pouring over room data sheets. The team had to make virtually all the decisions such as how far from the floor were the electric point to be situated. For each room the was a number of data sheets – one even detailing the number of coat-pegs on the back of the door with a diagram showing in plan, side view and elevation the positioning of one, two and three such pegs – such a waste of paper. These were the joys of designing a purpose built integrated unit. However with persistence and time an outstanding facility was agreed and built. There was an inpatient ward for nephrology patients; an inpatient transplant unit with four single rooms; an outpatient unit for nephrology, dialysis and transplant patients of four consulting rooms with en-suite examination rooms; a haemodialysis unit; a paediatric dialysis unit and a CAPD unit with additionally all the supporting services. There was no other facility in the UK providing such an integrated service. Although planning started in 1980 it was not till July 1992 that the topping out ceremony took place. The new facility was subsequently officially opened by the Duchess of Kent who spent considerable time talking with patients and staff. This renewed service worked well. The senior nurse was Anne Lewins, the adult dialysis area was managed by Charge Nurse Simon Sanasy, the outpatient area by Sister Georgina Speak.. Charge Nurse Haines continued to look after the paediatric section.
In the 1980s peritoneal dialysis became a reality for long term treatment due to the development of soft plastic catheters which could be tunnelled through the abdominal wall and remain in situ for prolonged periods. The technique of continuous ambulatory peritoneal dialysis was established and proved very successful. As a result a programme was developed involving a special team of nurses to train and subsequently manage patients. This facilitated a further expansion of the numbers of patients who could receive treatment. The programme was supervised by Dr Es Will and managed by Sister Bev Kingswood. This team functioned well in the new specifically dedicated peritoneal dialysis ward where there were rooms for training patients and their relatives as well as providing inpatient care for any intercurrent problems.
A Patients Association was formed in 1987 and this proved a useful forum to obtain the patients’ opinion on the service being provided as well as developing a self-help group. They have added much to the unit in addition to raising funds and awareness of renal diseases. Their motto is appropriately ‘An Association run by Patients for Patients’.
1992 was a time of the Bosnian war and the unit provided dialysis for one young boy who had somehow managed to travel from the Balkans to Leeds and was in desperate need of treatment. He had been orphaned and did not speak a word of English. He must have found it very difficult to come to terms with his circumstances. In the unit there was another patient from Bosnia receiving dialysis but she refused to speak with the young man because he was of the Muslim faith. This brought home to staff the very divisive nature of the conflict.
In 1993 Dr Chas Newstead was appointed from a Senior Registrar post in Manchester. He brought with him a particular expertise and interest in transplantation. He developed a programme for the detailed work-up of patients prior to transplantation which significantly improved results. This was a time when novel immunosuppressive agents were being introduced and experience needed to be gained into their effective and safe introduction to patient management. Another development which he pioneered was the living donor programme. A number of living donations had been performed but it had not been developed to its maximum potential.
During the 1990s the unit had advantage from a number of postgraduates coming from India. This functioned through the College of Physicians of Edinburgh by a scheme known as the Double Sponsorship Scheme whereby a consultant in the UK who knew a consultant in India could arrange for a junior trainee to come to the UK for further training providing that the consultant in India could assert that the trainee was of a standard to benefit from such training and was competent in English language. The further training usually lasted for a year, occasionally longer, and the majority returned home having benefitted from the scheme. Some have gone on to have distinguished careers to the benefit of patients in India. Unfortunately this arrangement was terminated by the Postgraduate Dean which was a loss to both Leeds and India.
There were a number of initiatives to increase the number of patients undergoing transplantation. In 1996 Prof Davison, as he was by then having been awarded a personal chair in renal medicine earlier in the year, was a member of a group of European Physicians involved in the management of patients with renal failure who were invited to Rome to discuss with Pope John Paul the benefits of transplantation. The message was to emphasise that the donation of an organ was an act of Christian charity and should be supported by the Catholic Church. This message was well received and, in some small way, helped the Roman Church to accept and promote transplantation.
Author: Sandy Davison
Specific remarks on Sandy Davison’s history on St James’s University Hospital Renal Unit – errata and expansions
By Es Will
- The number of grafts in 1994 at St James’s was not twelve – perhaps 1974? Prof Giles was appointed in 1973. He died unexpectedly in 1992, aged 55. A monkey puzzle tree in front of Lincoln Wing commemorates his link to the USA and Starzl.
- Notably, the excellent, later Indian trainees emigrated to rewarding careers in the USA, with Leeds as a notional stepping stone.
- Professor Davison modestly omits his Foundation Editorship of the EDTA Journal, Nephrology, Dialysis and Transplantation, in the mid-1980s, together with many other international appointments.
- The custom-built renal facilities in Lincoln Wing were always vulnerable to criticism over outpatient workloads, for example. The regional support role was used to justify that, particularly. As the haemodialysis patient number rose, two wards at Seacroft were converted to routine maintenance haemodialysis activity, but the amalgamation with the LGI exposed the need for more SJUH in-patient space. The other factor was a desired expansion of the renal transplant capacity, with live-donor, and later pre-end stage, recipients being accommodated. Newer immunosuppressives also reduced the need for routinely providing secluded post-transplant care. The functional integration of the unit was then somewhat compromised and the facilities more scattered, albeit locally in that area of the hospital.
- The early, makeshift, Bradford (pop 377k) and York (pop 142k) satellite functions were transferred subsequently to new, main hospital renal units, independent of St James’s, initially under Dr Robin Jeffrey and Dr David Worth respectively.
- The satellite programme from St James’s was accelerated after 1980 and came to include: Dewsbury (64k), Huddersfield (149k), Halifax (88k), Wakefield (353k), Seacroft and Beeston, Leeds (822k). Routine Management was through detailed monthly patient review (ca 40 each centre) at St James’s with the satellite senior nursing staff, supported by routine clinical IT exception reporting and graphical display. This was essentially a tactical, troubleshooting, patient management system. Patients visited SJUH OPD for strategic review periodically. Few consultant visits were required for secure clinical supervision.
- The satellite monitoring system reflected the limitation of senior staff appointments across the 1980-90s. When consultant numbers increased the uniformity of clinical management at satellites and main unit could not be guaranteed. That brought to an end a series of single centre RCTs of an adequate scale in renal anaemia, for example, the last being in 2005.(1)
- Whilst the satellite organisation of dialysis was not a new development, the ring of suitably sized towns around Leeds meant that a classic ‘hub and spoke’ system could be created, in contrast to the later ‘networking’ solution of metropolitan Manchester. The progressive satellite development was possible only through in-house technical set-up and support, which was compromised ultimately by the increasing sophistication of equipment and manufacturer maintenance. The recruitment and training of senior nursing staff for the satellites took the role of dialysis nursing to a further level of complexity, which they thoroughly enjoyed, extending the very early efforts at Guy’s and elsewhere.(2)
- Monthly reports of renal patient treatments and status were created on the clinical IT system and passed to hospital managers for years, but because their NHS funding model depended on a snapshot status they were never used to calculate the obvious costs of frequent transfers between modalities, etc.
To make the transfers more explicit and expose the scale of unit activity a diagram was used to show monthly transfers between modalities. This was a visual representation of a mathematical matrix.(3) The large number of treatment transfers are apparent in an early sample diagram, for example from Haemodialysis (H) to PD, with deaths in brackets (Figure 1).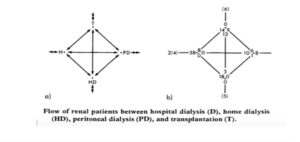
References
- Tolman C, Richardson D, Bartlett C, Will E. Structured conversion from thrice weekly to weekly erythropoietic regimens using a computerized decision-support system: a randomised clinical study. J Am Soc Nephrol 2005;16(5):1463-1470.
- https://ukkidneyhistory.org/themes/remarkable-people/remarkable-professionals/stewart-cameron/stewart-cameron-towards-an-intellectual-history/
- Dibble JB, Will EJ. Complex clinical workloads in a nutshell. Lancet 1984;2:134.
Last Updated on March 28, 2025 by John Feehally