Scribner shunt in the right ankle. This later design without baseplates was widely used for over 20 years.
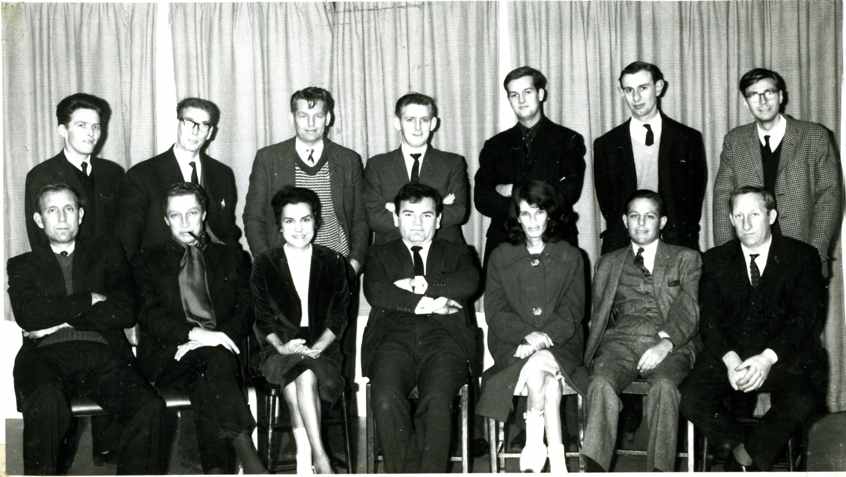
Image above: The ‘Lucky Thirteen’ at the Royal Free Hospital, 1965. See below.
In September 1960 Scribner recounted his first 6 months experience of dialysis via the new arteriovenous shunt (later often called a Scribner shunt) at the first International Society of Nephrology meeting in Evian, which had just launched its mineral water. (More on the international scene in Dialysis for endstage renal failure in the world from historyofnephrology.) The shunt was the first device to make repeated access to the circulation feasible – previously each dialysis had required surgical cut-down and cannulation of tubes into an artery and vein. It is remarkable that in 1960-62, when capacity for treating acute renal failure was still inadequate, some were already thinking of treating end-stage kidney disease. Most were not though. A symposium in Edinburgh in March 1961, when dialysis for AKI was still very new, was one of the first conferences to focus on kidney replacement therapy. Views expressed suggested that the general view was that Scribner’s experimentation with end stage renal failure was wild:
‘At the present time it is not known whether, given more efficient and practical machines, the life of the patient with chronic renal failure could be sustained indefinitely’ (Robson, Edinburgh) ‘In terminal renal disease … haemodialysis … only postpones the evil day and gives false hope to both patient and relatives’ (Parsons, Leeds)
Dialysis for end stage renal failure at the Royal Free
At the 1960 Evian meeting was Stanley Shaldon, then Sheila Sherlock’s Lecturer at the Royal Free Hospital in London. He had come to present a paper on diuretics in liver disease, but was impressed by Scribner’s presentation, and by another by Nils Alwall from Sweden, which hinted at the feasbility of long-term dialysis. The Royal Free Hospital had a dialysis machine, set up by urologist John Hopewell specifically to support patients with end stage renal disease in preparation for transplantation, which he was developing there with the aid of Roy Calne. However at this stage the machine had mostly been used for acute renal failure. It was established at the Lawn Road branch of the Royal Free, close to Urology (the transplanters) and the obstetricians who looked after women with septic abortion and other obstetric renal failure, who had been keen to have dialysis available. Transplantation had so far only been successful for identical twins but attempts using thiopurine soon followed.
A strong incentive to develop treatments for end stage disease must have been the powerful effect of patients with end stage renal disease arriving at renal units before the chronicity of their disease was recognised. Some had a few dialysis sessions, but treatment could not be continued because of inability to access the circulation repeatedly.
Early the following year Shaldon was allowed to test the technique he had used to study liver blood flow – Seldinger insertion of vascular catheters into femoral vessels without a surgical procedure – to connect patients to the dialysis machine. He went on to develop maintenance dialysis using this technique, and you can see a remarkable Movietone newsreel from 1963 describing this. The Royal Free became the first UK centre to systematically treat chronic renal failure by dialysis.
Intermittent dialysis catches on
The first episode of the BBC TV programme Tomorrow’s World in 1965 featured the Royal Free dialysis programme led by Stanley Shaldon (with Rosemary Baillod), and including some early home haemodialysis, and hospital footage. In the photo below, Shaldon is centre, front row. The longest survivor from the group, Robin Eady, is second from the right on the front row, next to Ray Jones (pictured on dialysis here).
The Royal Free Hospital’s ‘lucky 13’ with Dr Stanley Shaldon in 1965.
In December 1963 Newcastle became the second unit in the UK to start treating end stage renal failure by dialysis. At the second International Society of Nephrology meeting in Prague in 1963, Hugh de Wardener (Fulham/Charing Cross Hospital) found that Scribner’s patients were still alive. So he sent a team to Seattle to learn the technique. They returned to set up a unit specifically for long-term dialysis at Fulham Hospital (a branch of Charing Cross Hospital) in August 1964. This became the third unit providing dialysis for end stage renal failure in the UK, but the first set up to do only that. Several other units that treated ARF followed later that year. In 1965 Shaldon estimated that the 19 patients they were dialysing at the Royal Free were more than half of those kept alive by intermittent dialysis in the UK. By mid 1966 there were 104 patients.
Left: Dr David Kerr assembing a Kiil dialyser. Right: UK patients 1966.
Implementing this new treatment took ingenuity and experimentation, that included liberating staff roles to cross their traditional boundaries. This was experienced as liberating by dedicated staf, but often generated resistance from above. Physicians undertook minor vascular procedures, nurses cannulated, took blood, led dialysis, made decisions about treatment, and taught patients how to take it home.
This video (YouTube) from the EDTNA/ ERCA features Dr Rosemary Baillod, a junior doctor at the time, with dialysis nurses Ann Eady, Sally Taber, Lesley Pavitt, Joy Foo, and Marcelle de Sousa, talking about their roles, unimaginable when they first trained. More at Extending Professional Roles.
An accepted treatment
The speed of change was dramatic. In the first edition of deWardener’s book on the new specialty, The Kidney, in 1958, the treatment of terminal chronic renal failure was entirely palliative. It recommended using chlorpromazine, morphine and paraldehyde for symptoms. Just six years later, the second edition included discussion of peritoneal as well as haemodialysis, and of transplantation, with the prescient prediction that none of these would be able to meet the new demand for treatment. After the technical hurdles, and professional resistance, finance quickly became the third barrier.
Early expansion
The 1969 Edinburgh dialysis unit
Interior of dialysis unit. Note the Avery weighbeds, designed by Michael Darmady (see Units – Salisbury)
A working party established by the Department of Health, chaired by Hugh de Wardener who opened the unit at Fulham Hospital (a branch of Charing Cross) recommended the building of a 10-bedded renal unit in each health region in England and Wales to cope (more in National planning for RRT commences.). Scotland and Northern Ireland followed. The photos show the Edinburgh unit which opened in 1969. Thirty one units were built within 5 years – a great start, but indeed it did not prove enough. It was probably only in the 1990s that the UK completely caught up with providing dialysis for all those who could benefit. This progress would probably have been impossible if the results of transplantation had not improved beyond all recognition across the same period.
Challenges
This new technology and new group of patients surviving longer than ever seen before with renal failure presented new problems and dilemmas. These included technical issues related to the treatment (air embolus, blood loss, reactions to membranes and contaminants), as well as blood-borne hepatitis, and issues arising from water quality. More on challenges
Long term survivors on dialysis: Eady and some other long-term survivors (historyofnephrology) Papers from an advisory committee and working party to the Department of Health, 1960s, are in the National Archives Office at Kew. On paper, not digital, though some digitised for this project [More on this to follow].