National planning for RRT commences
A Department of Health Working Party
Haemodialysis as a treatment for end-stage renal failure did not start in the UK in a planned way. There was at the beginning no national policy, no central NHS view about its present and future role, and no allocated funding for infrastructure, staff or running costs.
Rather it began because committed enthusiasts saw maintenance HD might be possible, and set off to make it work, scraping together the resources from local, often charitable, sources.
As early as 1964, the Department of Health (DoH) realised there was an emerging challenge. Despite some professional scepticism, there was great public interest and more centres were beginning maintenance HD programmes. So in autumn 1964, DoH established a Working Party on Intermittent Dialysis for Chronic Renal Failure which met from 1965 to 1969; the minutes of the working party can be read in the National Archives at Kew.
To chair the working party, DOH chose Hugh de Wardener, professor medicine at Charing Cross Hospital, one of the earliest proponents of maintenance HD.
The contemporary reader used to the Renal Association, now UKKA, being asked for its expert advice on matters of policy and planning in kidney care, should be reminded that RA in the 1960s was still purely a scientific society for those interested in the kidney and kidney disease. It had no role, nor any aspirations, in advising on health policy nor in patient advocacy. de Wardener was invited as an individual to chair the working party, not a representative of any organisation.
It is also important to note that the remit of the working party was restricted to England and Wales and covered only dialysis in adults. There was no discussion of transplantation, and no mention of children.
The working party made rapid progress. In 1965 it made recommendations for ten to twenty 10-bedded units to be established across the UK, and by December 1965 the recommendations were accepted by ministers, with some central funding allocated.
The new units were all to be placed in teaching hospitals, and based in academic departments of medicine. The sites seem to have been chosen in part by established expertise and enthusiasm, and in part by the need to ensure units were geographically widespread.
Chosen units included some already active in the new treatment techniques (including for example Royal Free, Newcastle, Charing Cross, Edinburgh).
Others chosen units had relevant related experience and enthusiasm, though no track record in maintenance HD. For example Guy’s which had been using dialysis to treat acute renal failure for some years had a published research record in that field. The decision to place one of the new units at Guy’s had far reaching effects. A young Stewart Cameron had recently been appointed as senior lecturer to lead the development of renal medicine at Guy’s, but was so short of resources that he was considering moving elsewhere. The arrival of DoH funding changed his plan and he remined at Guy’s for 30 years to help develop a world famous renal unit.
Other units were placed in sites which were not notably active in renal medicine. In Wales for example, DoH chose Cardiff and approached the academic medical unit, led by haematologist Harold Scarborough. Although there was a single Kolff dialysis machine in Cardiff, the only person with any relevant expertise was a young SHO, Netar Mallick, who had qualified in Manchester, and come to Cardiff from Boston, USA, where he had published work on extracorporeal circuits for cardiac surgery. So Mallick found himself appointed by Scarborough at the age of only 28 to lead the development of dialysis in Cardiff, and represent Cardiff on de Wardener’s working party. (Mallick returned to Manchester and in due course became Professor Sir Netar Mallick, RA President and the first government advisor on renal disease).
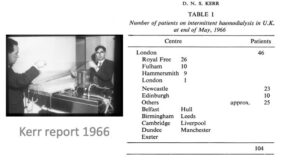
Progress in implementing the working party recommendations was rapid. By May 1966 15 units were established and over 100 patients were being treated, as documented by David Kerr (figure).
Although central funding was scheduled to end in March 1969, there were discussions underway about future funding models. There was much optimism. But then the expansion of maintenance HD was then derailed by the outbreaks of hepatitis B in renal units, leading to the deaths of patients and staff, which called to a halt any immediate hope of further growth, indeed offered an existential threat to maintenance HD in the UK.
Author – John Feehally
Last Updated on January 3, 2025 by John Feehally